Beyond the DSM: Neuro-affirmative Language for ADHD Diagnostic Report Writing
Why the language we use in diagnostic reports matters — and how it can begin a therapeutic journey.
Recently, I found myself reflecting on my own experience of being on the other side of a diagnostic assessment as a late-diagnosed adult.
What stood out most was the language used to describe my experiences. I remember how vulnerable it felt to tell my story openly — relaying moments where I had felt “incompetent”, “stupid”, or “silly” — words that had stayed with me over time. Sharing this felt delicate, almost like handing over something very personal and easily misunderstood. What mattered deeply was how those experiences were reflected back to me: held gently, validated, and understood using respectful language. I had not fully realised how worried I was that it would be framed as a deficit — that the report would reinforce the very shame I had carried for so long. I felt fortunate, as it turned out, to have a neurodivergent clinician assessing me. That made a difference.
That experience changed how I understand what assessment actually is — and what it could be. When you are the person being described, you notice things you might not have noticed before. Especially the language.
What diagnostic assessments are really for
Diagnostic assessments are not simply narratives. They sit within clinical frameworks that help people access recognition, support, and accommodations. Diagnostic criteria and structured processes serve an important and real purpose.
Yet within those necessary frameworks, there is still space for something else: careful attention to the language we choose, and the kind of story our reports tell.
Is an assessment simply a checklist against diagnostic criteria? Or could it become the beginning of a therapeutic journey — one grounded in compassion, understanding, and a clearer narrative of how someone's mind works?
What kind of story do we want our assessments to tell?
Acknowledging struggle without deficit framing
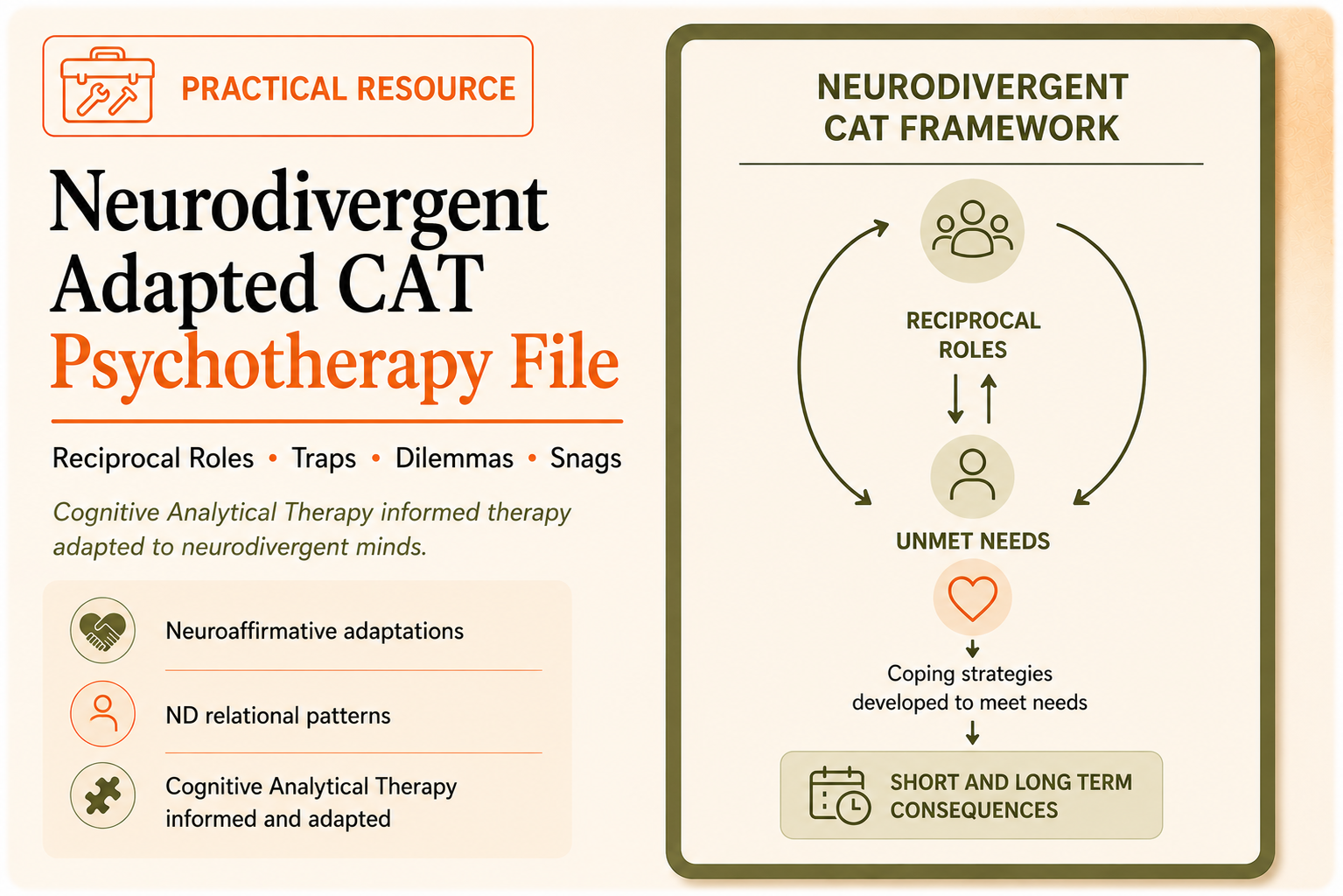
A neuro-affirmative approach aims to honour neurodivergent experience. It recognises strengths, differences, and identity, while also acknowledging the real challenges that arise when neurodivergent minds meet systems largely built for neurotypical expectations.
This is not about minimising difficulty. ADHD can bring real effort, limitation, and frustration — particularly within environments not designed for the way these minds work. Sometimes the very strengths of a neurotype become challenges when they are unsupported. A mind that generates many ideas can be creative and expansive, yet without the right scaffolding, may also lead to cognitive crowding or difficulty completing tasks.
Understanding the mechanisms behind these patterns often replaces shame with clarity. That shift — from self-blame to self-understanding — can begin in a diagnostic report.
When the system requires deficit language to access support
There is a deeper tension in this work. In order to receive recognition, support, or accommodations, people often need to move through frameworks built on deficit-focused language. Paradoxically, they may have to step into a system that describes them in terms of impairment in order to access understanding and validation.
Both the person being assessed and the clinician may be navigating a system that does not fully capture the richness of neurodivergent experience. Holding this balance — acknowledging genuine difficulties while offering a compassionate narrative — requires careful thought.
How report language can change what someone hears
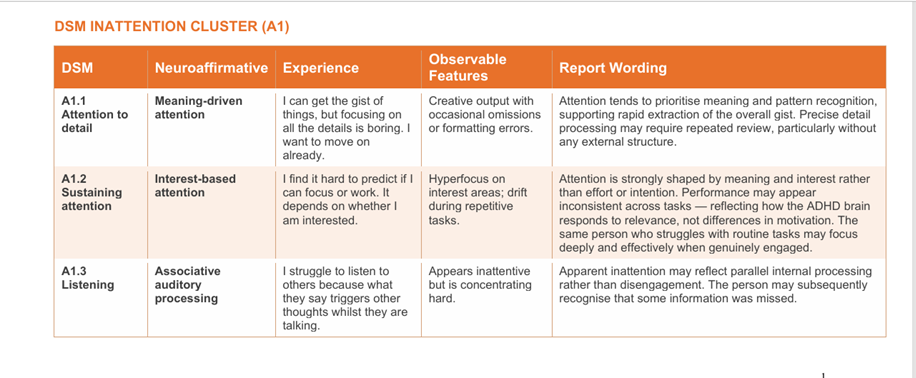
Experimenting with language in my own report writing has shown me that even small changes can make a meaningful difference — without sacrificing diagnostic clarity. The examples below are drawn from my neuroaffirmative ADHD language guide. Each says the same clinical thing, but locates the difficulty in a neurological mechanism rather than in the person’s character or intention. That distinction matters enormously to the person reading it.
Why this matters — and what clinicians can do
Small shifts in language cannot change systems overnight. They cannot undo years of being told you are lazy, difficult, or not trying hard enough. But they can change something important: how someone begins to understand their own story.
For many people — particularly those who reach assessment as adults, after decades of confusion and self-doubt — a diagnostic report is a document they will return to many times. It may be the first place their experience has been formally named, and named well.
That is not a small thing. It is an opportunity that belongs to every clinician who writes one.
We cannot always change the system. But we can change what someone hears when they read about themselves for the first time.
That is not a small thing. It is an opportunity that belongs to every clinician who writes one. I have started sharing a neuroaffirmative language table with other clinicians who are equally aware of this quiet responsibility. If you’d like a copy, it is available below.
Explore other resources