The Hidden ND-Clinician Trap: You’re Serving Everyone Except Yourself
Most of us built our practices to be safer, more honest spaces for neurodivergent clients. Grounded in neuroaffirmative principles. Reducing harm. Moving away from deficit-based models that never fit us either.
But there's a quieter truth underneath that.
Most ND clinicians struggle to extend the same scaffolding to themselves.
I know this professionally and personally — the specific point of feeling clinically successful and internally overwhelmed and mentally crowded at the same time, and having to work out, slowly, how to build a practice that is both ethical and actually sustainable. Not one that runs on willpower and overcompensates for executive difficulties.
This isn't a personal failure. It's a predictable pattern with a recognisable architecture. And unless it's addressed structurally, it leads somewhere most of us don't want to admit we're heading.
Why ND Clinicians Are Particularly Vulnerable
ND Clinians can bring a specific internal architecture. High compassion and striving for completeness/perfection that tips into chronic over-responsibility. Analytical depth that fuels perfectionist spirals. A strong autonomy drive that makes limit-setting feel like a values betrayal. Ethical standards so internalised that the fear of getting it wrong becomes its own background noise. Their special interest may be in their area of work which acts like a magnet.
None of these are flaws in themselves. They are often exactly what makes ND clinicians exceptional — deeply attuned, genuinely invested, intellectually rigorous.
But in the context of running a practice, they interact in a specific and predictable way.
It means you may build their practice around the needs of the community. Not the needs of the clinician in the room.
The outside looks like dedication. The inside feels like running on empty.
Three Traps Clinican’s can fall into
Ethical perfectionism
This isn't about having high standards. It's about standards that have drifted past what is actually achievable — and past what was ever necessary in the first place. The report rewritten five times. The session replayed on the drive home. The low, persistent sense that what you produced didn't quite meet the bar — a bar that moves every time you reach it.
For many ND clinicians, this has roots in neurodivergent patterns of attention to detail and constant idea generation, layered over a lifetime of compensating, masking, and needing to be correct to feel safe. The literature on autistic burnout and late-identified ADHD adults points consistently to this pattern — the cost of chronically overriding your own limits to meet an internalised standard that was never calibrated to how you actually function.
What shifts this isn't trying harder. It's externalising the structure. When the framework for a feedback session or a diagnostic report already exists — when the architecture is built into the tool rather than reconstructed each time — the perfectionist spiral has less to grip onto when there is less cognitive load.
Emotional labour
You are not just working. You are holding emotional weight. Your clients' histories. The systemic failures that brought them to your room. Often, your own lived experience intersects with theirs in ways that don't always clock off at the end of the session.
ND clinicians frequently have a lower threshold for vicarious distress — supported by the literature on interoception and emotional contagion — and a higher drive to do something about it. The clinical hour ends. The holding doesn't.
And because this labour is invisible — it produces no output, takes up no diary slot — it rarely gets designed around. It just accumulates.
What shifts this isn't better self-regulation. It's designing recovery and adaptations into the structure of the week rather than hoping it will fit in the gaps. Protected reflective time. Peer spaces where you are the person being held without excessive masking, not the one doing the holding. A schedule that honours the emotional labour involved.
Disguised executive dysfunction
The admin is delayed. The invoice writing has been put off for three weeks. The letters that require starting are painful to start. However, ideas on how to make the system keep coming up, opening up new loops and workstreams that will be forgotten due to other cognitive load.
This is not laziness. It is the real cost of task initiation difficulties, context switching, and the invisible cognitive weight of running a practice on top of doing the clinical work. For many ND clinicians, this is the source of the deepest shame — because it sits in such sharp contrast to clinical competence. You can hold a complex formulation effortlessly and still find it genuinely hard to send a routine email.
That contradiction is worth naming directly: it isn't an inconsistency. It's the predictable presentation of executive dysfunction and variable energy and attention in a high-functioning context. What shifts this is reducing the number of decisions required to produce something clinically rigorous — a structure and adaptations that do some of the cognitive work for you. The shame-competence gap starts to close. Not because your identity has changed, but because the evidence against the shame narrative has.
Designing a Practice That Protects your capacity and Fits our Brain Style
The goal is not to fix yourself. It's not even to get better at running a practice. It's to design a practice that fits the brain you actually have — one that builds structure around how you function, rather than asking you to override yourself to function.
That reframe matters. The moment you stop treating your needs as inconvenient and start treating them as design requirements, the whole thing changes shape. These aren't productivity hacks. They aren't shortcuts. They are access needs — and your practice is allowed to be built around them, the same way you'd expect for any of your clients.
In practice, that looks like clear pathways instead of every task starting from scratch. Templates that carry some of the cognitive load for repeated work. Scheduling that reflects the energy you actually have, not the version of yourself that exists on your best week. Flow through the week with changes in tasks and recovery slots. Admin support where possible. Peer structures that hold you and where you don’t have to mask. Tools that reduce the decision load on work that shouldn't be costing you this much.
None of this is indulgent. It's what it takes to do the work well, for longer, without burning out the person doing it.
Scaffolds for ND Clinicians
I've built a set of neuroaffirmative scaffolds specifically for ND clinicians working in private practice — not because they solve everything, but to reduce the cognitive cost of the administrative and documentation work, creating more capacity for the reflective work. Templates and workflow structures. This is where capacity increases, from what becomes possible when the tool is doing some of the heavy lifting.
Some examples related to therapeutic diagnostic work for that i have found useful can be found in my Resource library. They include free Structured Feedback Session guide, neuroaffirmative Autism and ADHD feedback protocols — clear, collaborative, and ready to use without rethinking each time.
The free AI Diagnostic Formulation Summary template gives you a starting framework for feedback sessions that is neuroaffirmative, strengths-based, and clinically grounded — so you're not starting from a blank page.
The ND Profile Feedback report — covering autism, ADHD, and AuDHD — is a complete, structured report template aligned to DSM-5-TR and NICE NG87, AI-guided and human-reviewed, built to reduce the rewrite cycle without reducing clinical quality.
These aren't solutions to burnout. But each is one less thing you have to rebuild from scratch — and that matters more than it sounds.
If this resonates and you want to think through what a more sustainable practice structures have a browse.
Free neuro-affirmative assessment session setup guide
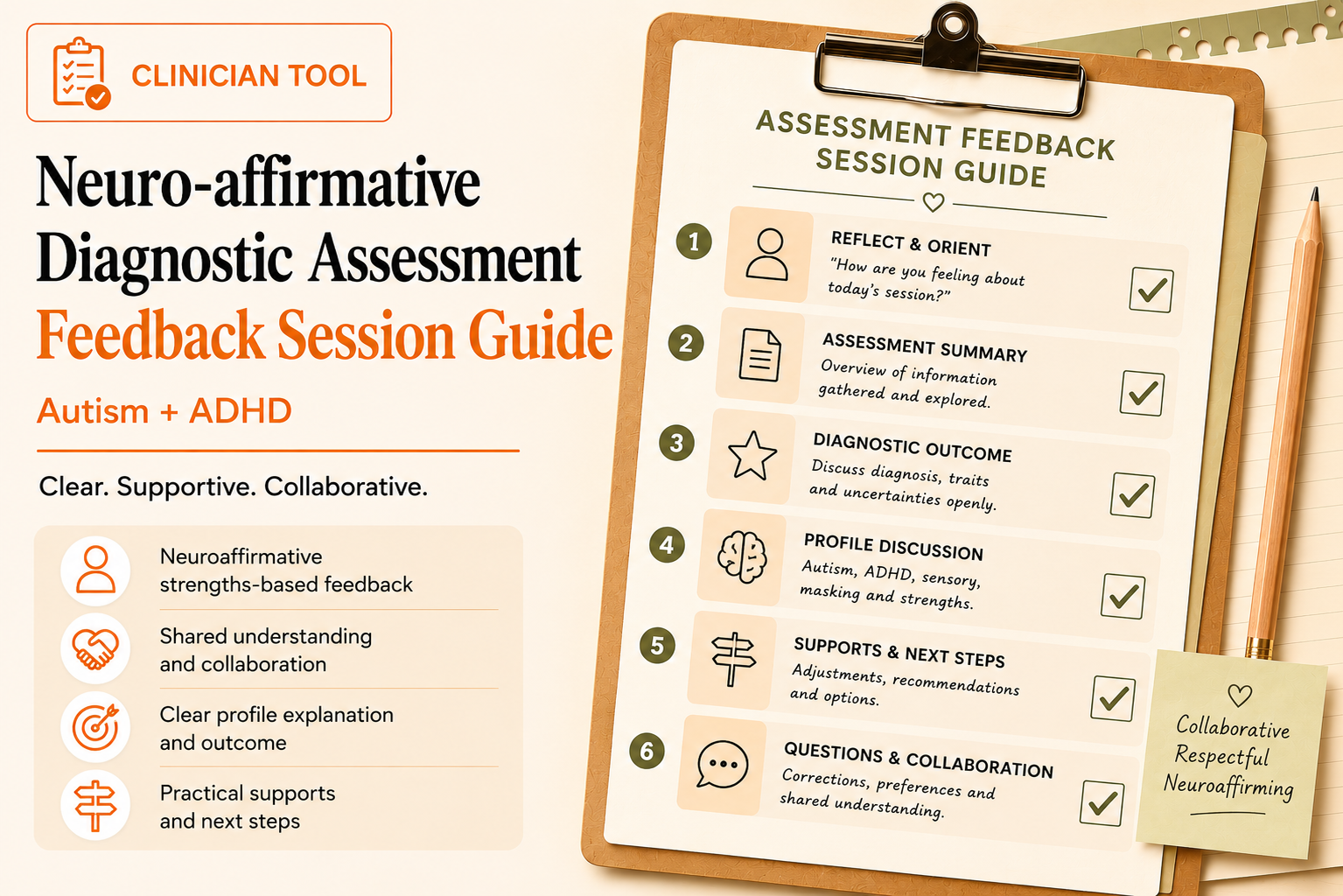
Free neuro-affirmative Diagnostic Assessment Feedback Session Guide
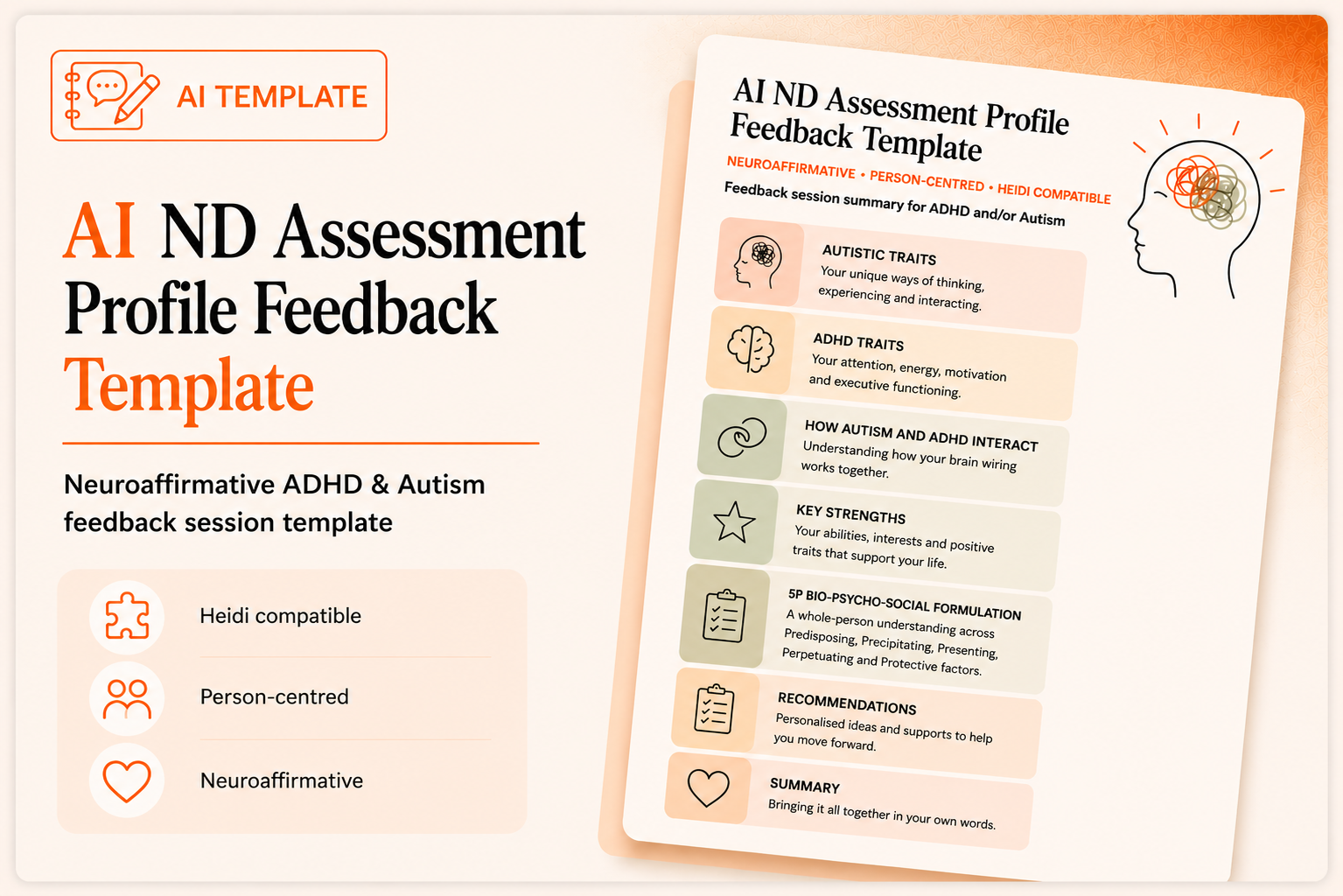
Free AI ND Profile feedback template
Shop the resource

Includes
Neuro-affirmative AI ADHD Diagnostic Assessment Report Template in 3 parts with instructions to use for AI Heidi Health.
Produces comprehensive neuro-affirmative reports which are DSM aligned include Diagnosis and Psychological Formulation in the Summary and Conclusion section.
Is based on current research and lived experience of adult late diagnosis.
Best for use in therapeutic Assessments utilizing rich information gathered via screening (PHQ-9, GAD-7, PCL-5CAARS, ASRS, WURS etc Optional), interview (DIVA/ACE), developmental tools (developmental history, direct observation, clinical interview, collateral information)
It details differential diagnosis, functional/contextual formulation and includes masking, trauma, ADHD, Autism, Learning Disability, culture, gender, and mental health
Includes a structured neuro-affirmative adult ADHD Diagnostic report template in Microsoft Word with References to copy and paste.
Requires proof reading and editing by a clinician as AI can make mistakes.
Explore other resources